The surgical techniques for ear reconstruction have been developed, so this is a plausible project.  The difficulty is finding the appropriate medical assistance to realise it. Since 1997, there were several instances where doctors initially expressed interest in assisting, but then changed their minds. The difficulty is finding the appropriate medical assistance to realise it. Since 1997, there were several instances where doctors initially expressed interest in assisting, but then changed their minds. The problem is that it goes beyond mere Cosmetic Surgery. It is not simply about the modifying or the adjusting of existing anatomical features (now sanctioned in our society), but rather what's perceived as the more monstrous pursuit of constructing an additional feature that conjures up either some congenital defect, an extreme body modification or even perhaps a radical genetic intervention... Constructing the Extra Ear would involve a number of procedures, over approximately 8-10 months. Techniques from Cosmetic, Re-constructive and Orthopedic surgery are necessary. The essential steps would be: - Harvesting cartilage from the rib cage.
- Carving the cartilage in the appropriate shape to provide the ear framework
- Positioning the shaped cartilage beneath the skin
- Lifting the ear form (the ear would be supported away from the side of the head with a cartilage wedge)
- Covering the skin defect with a full-thickness skin graft.
- Forming the ear lobule (this being done using local soft-tissue flaps with some internal cartilage support- otherwise atrophy of the lobule will occur)
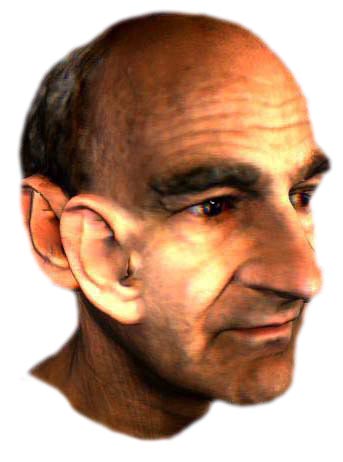
The lifting of the ear form and the lobule construction would be done 4-6 months after the cartilage has been placed beneath the skin. Alternatives to using cartilage are silicon implants or surgical implant material such as Medpor, which is a porous polyethylene substance. The advantage of Medpor over silicon would be that it allows vascularisation and ingrowth of tissue into the implant. Cartilage is preferable, but it requires an operation under general anaesthesia. Although the chosen position initially was in front of and beside the right ear, this is neither the safest nor the surest place anatomically to position it. (There are problems with facial nerves and the jaw-bone!). It would be more plausible though to place it beside but behind the right ear. The easiest and perhaps most practical to achieve  would be the construction of an EAR ON AN ARM. The skin of the forearm is smooth and would adequately stretch without the necessity of any inflating prosthesis (as might the the skin of the scalp area). It would be safer and would involve less surgical procedures. And disconnected from the face, the EAR ON AN ARM could be guided and pointed in different directions. (I would always have something up my sleeve). would be the construction of an EAR ON AN ARM. The skin of the forearm is smooth and would adequately stretch without the necessity of any inflating prosthesis (as might the the skin of the scalp area). It would be safer and would involve less surgical procedures. And disconnected from the face, the EAR ON AN ARM could be guided and pointed in different directions. (I would always have something up my sleeve). The mechanical fingers of the THIRD HAND counterpoint the soft and more dextrous fingers of the real right hand. The EXTRA EAR would mimic the actual ear in shape and structure and in addition it could have different functions. Imagine an ear that cannot hear but emits sounds. With an implanted sound chip and a proximity sensor it would speak to anyone who would get close to it. (Or if no-one got close it would whisper sweet nothings to the other ear anyway). Also, connected to a modem and a wearable computer it could broadcast RealAudio sounds to augment the local sounds that the actual ears hear. The EXTRA EAR becomes a kind of Internet antenna that telematically and acoustically scales up one of the body's senses. But these functional possibilities are not what justifies or authenticates the project. It would be interesting even without any utilitarian use. Why construct an ear? The ear is a beautiful and complex structure. In acupuncture, the ear is the site for the stimulation of body organs. The ear not only hears, but is also the organ of balance. To have an extra ear points to more than mere visual and anatomical excess.
ACKNOWLEDGEMENTS
THIS PROJECT WAS INITIATED DURING STELARC'S RESIDENCY AT THE ART DEPARTMENT OF CURTAIN UNIVERSITY OF TECHNOLOGY, PERTH IN 1997. ADVICE WAS SOUGHT FROM THE ANATOMY AND HUMAN BIOLOGY DEPARTMENT OF THE UNIVERSITY OF WESTERN AUSTRALIAN, ESPECIALLY FROM DR. STUART BUNT. THE LASER SCANNING OF THE HEAD, FOR THE 3D MODELLING OF THE EXTRA EAR WAS DONE BY JILL SMITH AND PHIL DENCH OF HEADUS. WITH THE ASSISTANCE OF DR. RACHEL ARMSTRONG, THIS PROJECT WAS PRESENTED TO THE MONTHLY GATHERING OF CONSULTING SURGEONS AT THE GRAND ROUND, JOHN RADCLIFFE HOSPITAL- OXFORD UNIVERSITY ON THE 5TH MARCH, 1999. |